
























Life after Injury from Landmines—in Colombia
Inequality as the Root of Violence
In the beautiful equatorial nation of Colombia, armed violence has increasingly become a way of life—and for many, a way to death or disability. Different factions, vying for money, power, drug trade, or redistribution of land and governance, have been at each other’s throats for decades. As a result, countless innocent persons, many of them women and children, have had their bodies, lives and dreams torn to shreds.
Violence in Colombia has been exacerbated by what is called “development aid” from the US government, much of it in the form of weapons and instruments of war. Officially this weaponry has been given to Colombia’s armed forces to fight the “War on Drugs.” The fact that Colombia’s military has a long track record of brutal human rights abuses and of alliances with the drug cartels has little relevance in this pervasive mission.
It is common knowledge that the underlying reason for the multibillion dollar flood of US weapons to Colombian military—and para-military—forces is to maintain the economic and political stability of Colombia’s pro-US oligarchy, i.e. to protect the properties and interests of wealthy landlords and transnational corporations. In practice, this translates into fighting the guerilla movements as well as crushing popular uprisings that demand agrarian reform and a more accountable, socially progressive government.
Similar to so many other countries that have a huge foreign debt, Colombia has been obliged to adopt “structural adjustment” policies imposed by the World Bank and IMF. These policies—including privatization of public services, cutbacks in welfare, and freezing of wages while freeing of prices have caused a deepening of poverty for millions of people, and have exacerbated migration of the landless to urban slums, with high rates of unemployment and homelessness. The desperation and hopelessness of young people has driven many to join the warring factions or turn to drugs and crime. All this has accelerated the vicious cycle of physical and structural violence. Nevertheless, many groups and communities are doing their best to cope with the difficulties and impove their situation.
Visit to Bogota on Invitation from CIREC and ICES
In May 2003, I (David Werner) was invited to Colombia by two local non-government groups with overlapping concerns. Both groups work to encourage the inclusion and increase the opportunities of marginalized persons and communities, through their active involvement with Community Based Rehabilitation (CBR).
The first group is CIREC—Centro Integral de Rehabilitación en Colombia. Based in Bogota, the program is now introducing Community Based Rehabilitation activities in rural areas. CIREC is exploring ways to include persons disabled by landmines in this enabling process.
The second group is ICES—Instituto Cerros del Sur—a community-run development, health, and rehabilitation program that aims to train disabled persons and street youth to become neighborhood health workers.
Training Landmine Amputees as Community Rehab Workers
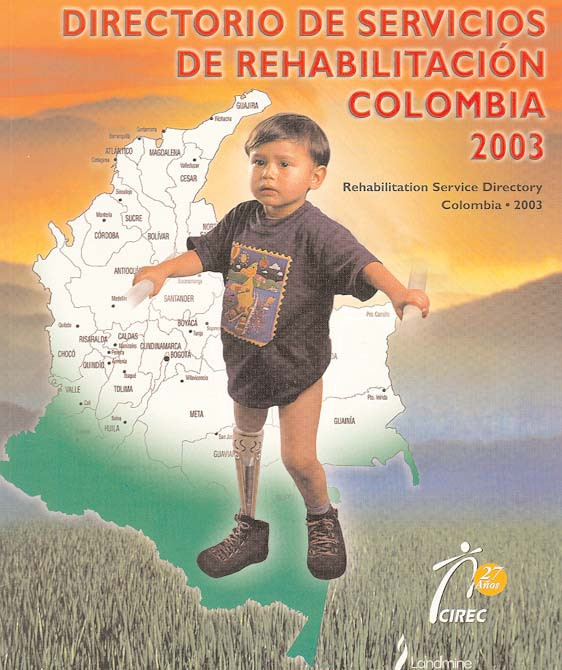
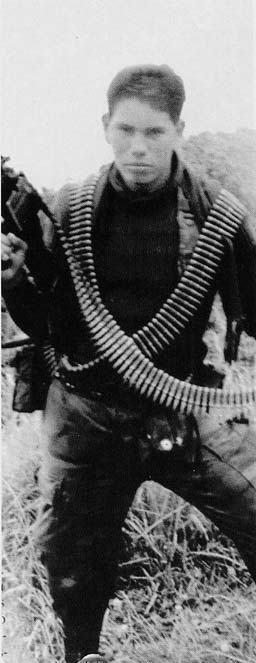
Most of us don’t think of Colombia as a country ravaged by landmines. But it is. Landmines in recent years have caused loss of limbs in over 1,300 people in Colombia. Some were involved in the fighting: i.e. soldiers, paramilitaries, guerillas, and drug dealers. But a substantial number are innocent victims of “periferal damage”: women, children, and farmers who happened to be in the wrong place at the wrong time.
Reportedly, nearly all the landmines deployed in Colombia are small handmade, hair-triggered devices produced by the guerillas. But who knows? Landmines remain a profitable item in international trade, with US corporations as the world’s biggest supplier. The US government still refuses to sign the international treaty banning landmines.
As the primary supplier of artificial limbs in Colombia, CIREC is painfully aware of the damage caused by landmines. Most of the persons disabled by mines are unemployed, often abandoned, and destitute.
CIREC is always looking for ways to make its services more accessible to the poorest people. It has developed many innovations in “assistive technology,” including low-cost shop-made knee-joints, that function remarkably well. CIREC realizes that an artificial limb is just the first part of rehabilitation for persons traumatized by landmines.
A number of the staff and technicians of CIREC are disabled themselves, some of them from landmines. The program is always looking for ways to gain fuller inclusion and more opportunities for disabled persons, in schooling, work, and community involvement.
A National Symposium on CBR Involving Victims of Landmines
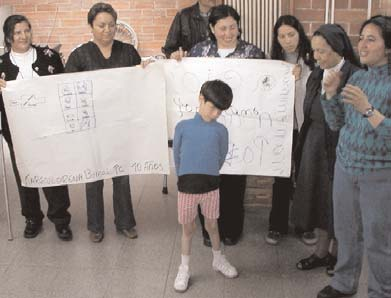
In May, 2003 CIREC organized a national “Symposium for Survivors of Landmines” to help them explore a new start on life.
Of the 200 participants present at the Symposium in Bogota, 70 were amputee victims of landmines. They ranged from 12 to 70 years old. Some were ex-soldiers, some paramilitaries, some drug growers or dealers, some guerillas, and still others were combinations of the above. Many had been on opposing sides of the violent confrontations.
Whatever faction the mine-injured persons came from, their disability was in some ways “the great equalizer.” At the CIREC Symposium they were all drawn together by what they now had in common: the loss of limb and livelihood. Rather than feeling the tension of opposing sides, the gathering seemed like a big family reunion.
One of the goals of the CIREC Forum was unique, and this was the reason why I had been invited. The managers and staff of CIREC (some disabled themselves or parents of disabled children) are interested in training landmine survivors as workers, technicians, and leaders in the budding Community Based Rehabilitation movement in rural areas. CIREC is helping to get CBR programs started in rural areas, and believes disabled persons should play a key role. A central purpose of the Symposium was to expose the 70 landmine-injured participants to their potential role as CBR workers, and excite them about the possibilities.
Whatever warring factions the landmine survivors came from, their disability was in some ways ‘the great equalizer’
That was my primary assignment. PROJIMO in Mexico has become renowned as a CBR program run and staffed by disabled villagers themselves. My role at the Symposium, therefore, was to communicate both to the rehab professionals and landmine injured participants the enormous potential of disabled persons as leaders and service providers in the CBR process.
I did my best. With the help of a Power point projector donated by Stichting Liliane Fonds in Holland, during the 3 day Forum I presented a potpourri of “slide shows” on many aspects of PROJIMO. I also described other community based programs in which disabled persons take the lead. I provided a range of stories and examples in which disabled rehab workers with limited formal education, by working in partnership with their clients, have achieved better, cheaper, more functional solutions than have highly trained, non-disabled experts.
|
|
|
The response was enthusiastic. Several of the landmine victims are eager to become community-based rehabilitation workers. Many professionals who attended the Forum said they now have much more interest in providing training, back-up and support to disabled community rehab workers.
Arrangements are presently being made for a few of the mine-injured trainees to apprentice in the prosthetic and brace-making shops at CIREC. Others will enter CBR training courses in their provinces. These disabled apprentices plan to return to their community as “multipliers,” teaching others what they have learned.
This venture, if successful, will provide an important breakthrough in terms of disabled persons taking a leading role in Community Based Rehabilitation initiatives.
Ciudad Bolivar: ‘Cerros del Sur’ Integrated Development Program
Of Bogota’s 8 million inhabitants, more than half live below the poverty line, earning less than US$2 per day. Roughly 2 million live in Ciudad Bolivar, a giant low-income squatter settlement plastered against the steep slopes of the hills flanking the mushrooming city. The closest parallels are the precarious hillside favelas of Sao Paulo and Rio, in Brazil.
The houses of Ciudad Bolivar are mostly hazardously constructed of big thin bricks cemented together vertically to save costs. Some dwellings have been propped up by poles as the hillside erodes from under them. There has not been a major earthquake for more than 40 years, but if one ever comes the death and disability tolls will be enormous.
In the past few years, declining wages and cutbacks in public services have caused increasing hardship in the city and country as a whole. But in one part of Ciudad Bolivar, called Cerros del Sur, the health and living conditions of the inhabitants have been gradually improving. These improvements are the result of a unique community-wide initiative called ICES, or Instituto Cerros del Sur. It was started by a group of local activists, concerned school teachers, and anthropologists who have involved the people in building and running an ambitious community program for “integral development.”
Built by the people themselves, the large blue center on the hillside caters to the needs of those who so often fall between the cracks. It is a health care facility, rehabilitation center, and income-generating training center all rolled into one. It primarily serves unemployed persons, single mothers, and children who for reasons of poverty or disability have trouble gaining entry into the state schools.
Disabled Persons and Street Youth as Community Health Workers?
In Ciudad Bolivar as in most of Colombia government health centers are few and far between. Service fees keep rising as the supply of useful medicines keeps shrinkng. Public hospitals are being privatized, pricing their services out of the poor’s reach. For many people the right to basic health care has become empty rhetoric.
ICES is collaborating with a pilot venture called the “Model for Community Integration of Persons with Special Needs,” coordinated by Ashoka fellow, Tatiana Gomez Duran. In this model, an effort is made to integrate disabled and marginalized persons into respected service-providing roles in the community.
One purpose of my visit to Ciudad Bolivar was to explore the possibility of training street youth and disabled young persons as community health workers. This plan of enabling the neediest people as service providers parallels CIREC’s plan to train landmine victims as community rehabilitation workers.
I was delighted to learn that the inspiration for both these plans to train and empower marginalized persons as service providers came in large part from the example of projects Piaxtla and PROJIMO in Mexico, about which the facilitators in Colombia had read in our books (Where There Is No Doctor and Helping Health Workers Learn, as well as Disabled Village Children, and Nothing About Us Without Us). I am constantly amazed at how wide the impact of these books is, and how many innovative and empowering initiatives they have helped trigger. (Where There is No Doctor is now in over 90 languages.)
As in the CIREC Forum, the staff, families, and young people involved in the Ciudad Bolivar initiative were enthusiastic, and the prospects for launching a highly participatory community-based health initiative look very promising.
A Hands-On Workshop: Making Assistive Devices for Disabled Children
CIREC and ICES—the two groups that invited me to Bogota—joined together to organize a full day hands-on workshop in appropriate assistive technology. Representatives from both programs took part. Altogether there were about 30 course participants, plus 7 disabled children and their family members. Participants were selected with the idea that they would later function as teachers or “multipliers,” sharing with others what they would learn. Included were several of the landmine amputees, an assortment of rehab professionals, and a number of facilitators and young trainees from ICES. A valuable addition to the motley group were 5 nuns from programs that help disabled children, and who are “mediators” for assistance from Stichting Liliane Fonds in Holland.
The workshop was held at the CIREC Rehab Center in Bogota. As facilitators, CIREC staff—disabled and non-disabled—had generously gathered together the necessary simple tools and supplies. For teaching purposes, UNICEF filmed the entire workshop.
Several days before the workshop I had joined some of the participants in visiting the homes of disabled children for whom we would be making assistive devices. Home visits are essential for understanding the environment where the children live.
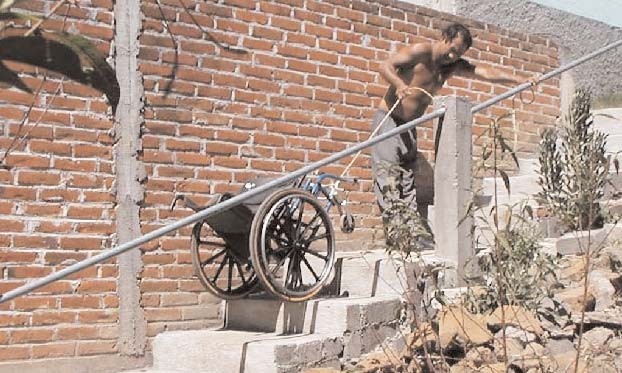
Participants can explore with the children and their families how to design an assistive device according to the unique limitations and possibilities in the home and community. For me as a stranger to the area, these home visits proved enlightening. We found that for many of the children and their families the biggest problem was accessibility. For example, two brothers with muscular dystrophy lived in a cramped hut on a steep hillside. They had to climb nearly 50 steps to reach the front door. This made wheelchair accessibility almost impossible. Any form ofmobility for persons who can’t walk would be a major challenge.
During the workshop participants divided into 7 small groups. For broader exposure, persons from the same program were placed be in different groups. Each group worked with one child and his or her family member(s).
The Goals of the Hands-On Assistive Technology Workshop
-
Demystify the process of making simple but functional aids,
-
Encourage innovative problem solving as a group process,
-
Observe how important it is for rehab workers to interact with family members and disabled children as partners and equals in the problem-solving process,
-
Utilize local low-cost materials and simple tools in the creation of useful devices,
-
Find out ways to adapt to the limitations and possibilities of the individual child and family in the environment where they live,
-
Discover that making simple aids as an interactive process can be an exciting adventure,
-
Look for ways to make assistive or therapeutic devices that are functional and fun,
-
Learn collectively from our successes and mistakes.
The 6 Stages of the Workshop
-
Pre-workshop home visits: Each small group visits the home of the child it will be working with, to make friends with the child and family and to observe possibilities and limitations. They listen to what the child and family say they want and need, and discuss/explore possible solutions and relatively simple technical aids.
-
First hour of workshop: design. Each group —including the participants, child, and family member(s) —designs the assistive device(s) they plan to make, and makes line drawings of it on large poster-paper.
-
Initial plenary session: Each small group presents and explainsits plans, shows its designs, and identifies the local, low-cost materials it intends to use. The larger group provides feedback and suggestions.
-
In the shop: Each small group constructs the assistive device, working closely with the child and family, in a trial and error approach. They use whatever local materials (cardboard, boards, plywood, string, paste, etc.) and simple tools are available.
-
Closing plenary: Each group, with the child and family member central to the process, presents the assistive device and how it helps the child (if indeed it does). In a sort of all-group evaluation, further suggestions are made.
-
Post-workshop follow-up: It is important that when the aid produced is inadequate or incomplete, that the program organizing the workshop makes sure there is adequate follow-up so that the child and family end up with something that really helps them do things more easily and enjoyably.
Helpful Suggestion: When Choosing the Children to Make Aids for this Kind of Workshop
-
Select children who can benefit from a simple device that can be made with local low-cost materials in 2 to 3 hours,
-
Select at least some children who can express their wishes, so the child herself can participate in the problem-solving process (and perhaps in making the device),
-
Choose children who get along well with strangers, who are cooperative, and who are likely to enjoy all the attention and to endure the long session. (Be sure to make provison for naps, refreshments, food, and quiet-time, as needed),
-
Select children who have a wide range of problems and needs, so that a spectrum of different assistive devices can be made and presented by the various small groups,
-
Try to choose children whose parents are eager to participate in the workshop and are prepared to contribute as equals in the problem-solving and aid-building process.
Examples of Assistive Technology Designed and Made for Children in the Bogota Workshop
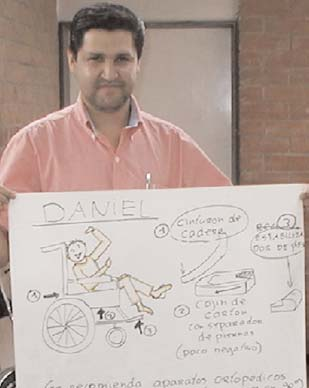
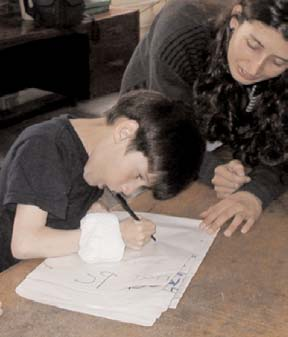
Daniel
Daniel is a 10 year old boy with cerebral palsy. We first visited him in his home (photo on right). Daniel is fairly intelligent, but has a hard time forming words. Mostly with gestures, he indicated that what he wanted most was to be able to do more things for himself, like sit upright and eat and draw.
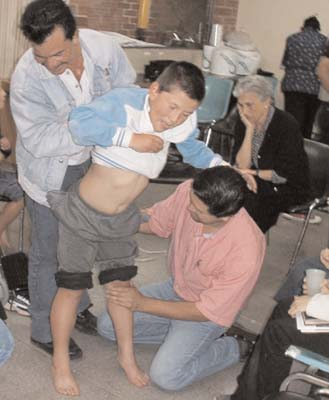
The combination of athetosis (involuntary movements) and spasticity made it very difficult for Daniel to sit in his ill-fitted (donated) wheelchair. His legs and back would stiffen suddenly and he would slip forward out of the chair. The slippery canvas seat was so streched in front that it sloped downward, acting like a slide.
In the workshop, the group working with Daniel examined and evaluated his needs and possibilities, with his and his mother’s help. They found that by stabilizing his legs with the knees bent back slightly, under the seat, he had much less spasticity (uncontrolled stiffening) in his legs and whole body.
They drew up a plan for modification of the wheelchair. This included:
-
reclining the seat backwards
-
a separator between his knees
-
a seat belt at 45 degrees, low and tight
-
footrests and leg supports to hold his knees at less than a right angle.
|
|
|
Karen
Karen is a bright, very active little girl with athetoid cerebral palsy. She cannot speak but communicates well with her own sign language. She does most things well and goes to school. But she has trouble writing and drawing because of the uncontrolled motion of her arms. Her group decided to make her a “communication board” with pictures, words and hand signs to help her express her needs better and to learn to read and sign.
|
|
|
Jose and Alan
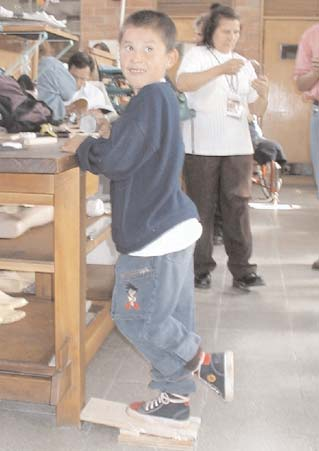
Jose and Alan, 8 and 12 years old, are two brothers with muscular dystrophy. We first visited them in their hillside house, climbing 50 steps to get there.
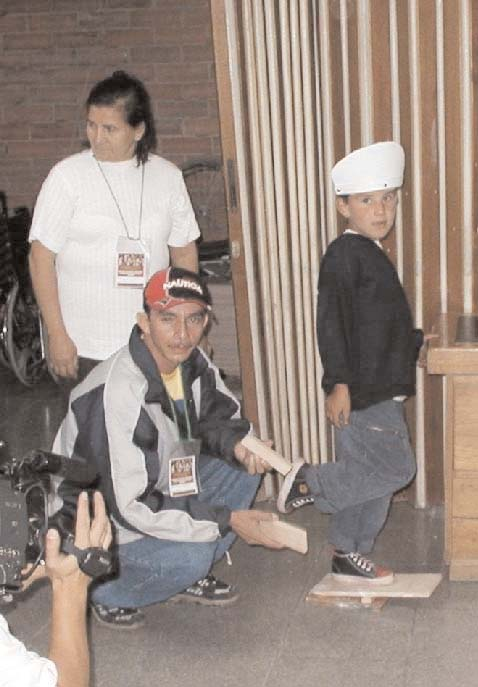
Alan can no longer walk and Jose has increasing difficulty. He is developing contractures in his heel cords. Given the difficult access to the home, it is especially important that he retain his ability to walk as long as possible—and that is his biggest wish.
With his weak legs Jose falls and hits his head so often that he has swellings, like little horns, on each side of his forehead. Because of his fear of injuring his head he doesn’t walk as much as he needs to to keep fit.
|
|
|
With the help of his father, the group also made for Jose a device to help him stretch his tight heel cords. It is a wooden wedge on which he bears his full weight first on one foot, then the other. The angle of the wedge can be gradually increased as his heel cords stretch. This exercise should help prevent contractures and keep Jose walking longer.
Alan is probably beyond walking, but has other pressing needs. He gets colds, sometimes pneumonia. He has trouble coughing up phlegm. He needs deep breathing exercises to improve his lung capacity and cough better.
|
|
|
To strengthen his lungs in a fun way, the group had Alan blow whistles and flutes. They also made a “blow toy” with a plastic bottle and straw, with bits of foam plastic in the bottle. The two boys can play to see who can lift the “snow storm” higher. The exercise may help both boys live longer.
Fernanda
Fernanda is a 5 year old girl who has spina bifida and and a severe spinal curve. The huge donated wheelchair in which she slumped was worsening the curve.
Fernanda herself helped her group design an insert for her wheelchair to help her sit in a better position.
The foam back is sculpted to protect her back and help prevent the curve from worsening. With her new seat Fernanda sits in a much better position and feels more comfortable. This will slow the collapse of her spine and perhaps add years to her life.
|
|
|
David
David is a 13 year old boy with spasticity who can walk holding on to something, but with knees bent from contractures.
David’s wheelchair is too wide to fit into the bathroom. The group thought to make him a narrow wheeled stool, but his foster father suggested putting a railing from the doorway to the toilet. “That way he will practice walking whenever he needs to go.”
With the foster father taking the lead, the group made a night-splint out of a strip of strong plastic. The spring-like action of the plastic gently helps to straighten David’s leg. The group learned the importance of teamwork.
Update on PROJIMO
Update 1: PROJIMO Coyotitan and Duranguito
Both PROJIMO programs, in their new, more accessible locations of Coyotitan and Duranguito, north of Mazatlan, Mexico, have been greatly extending their outreach. This is true not only for service coverage, but also spreading the message and methodology of Community Based Rehabilitation in which disabled persons themselves take the lead.
Part of this outreach is through exchanges with other non-governmental community programs. But increasingly, different government initiatives—municipal, state and national—are taking increased interest in learning from PROJIMO and applying its approach more widely.
At the same time, both PROJIMO programs have recently been receiving more assistance from the local and state government in building new, much needed facilities. Especially important in this regard are guest quarters, now that the number of apprentices (mostly disabled) from other programs is increasing.
The PROJIMO Rehabilitation Program in Coyotitan has received 10 brand new computers from the local government. These are being used not only for communication with a network of other programs, but also for income generating activities, including training of village girls and a “cyber-cafe.”
The PROJIMO Skills Training and Children’s Wheelchair Program in Duranguito has made a real breakthrough in terms of convincing the health and rehabilitation establishment that children need and have a right to wheelchairs and equipment that actually fit them and help them function better. Requests for personalized wheelchairs and—more important—request to help train local teams of disabled wheelchair builders, are now coming in from several states.
Both government and private donors are helping PROJIMO Duranguito with part of the cost of building its new workshops and quarters on land donated by the village. Efrain Zamora—a helper at PROJIMO since he was a boy and who has recently been studying alternative architecture, is helping to design low-cost, environmentally friendly buildings.
Update 2: A Meeting and Network of Programs and Mediators Assisted by Stichting Liliane Fonds (SLF)
For many years children assisted by PROJIMO have received financial help from Liliane Foundation in Holland (SLF) in meeting their disability-related needs. Two of PROJIMO’s long-time disabled leaders, Mari Picos and Gabriel Zepeda, are now “mediators” with Liliane in this process.
Over the years, PROJIMO has helped or inspired a number of other community rehab programs to get started in various parts of Mexico. Many of these programs now also get help for disabled children through SLF.
In March, 2003, Hortensia Uribe Sierra, Latin American coordinator from SLF, visited SLF-assisted programs in Mexico. With the help of David Werner and Dolores Vicencio of PROESA, she organized an “Ecuentro” (Encounter), inviting all of the Mexican SLF mediators. Hortenisa and David also visited several of the six SLF-assisted programs.
Update 3: Revival of the CBR Network
The Encuentro, held at the PROESA CBR program in Michoacan, was very productive in terms of sharing methods and arranging future interaction. It was agreed that different programs have different skills and strengths. We all have a lot to learn from each other. We decided to reactivate a network of Community Rehab Programs that we had started years ago but had gradually disappeared due to economic constraints.
To get the ball rolling, we made plans for several cross program apprenticeships. In fact, for the past 3 months a young man from PROESA who is parapelegic, Jose Luis, has been at PROJIMO learning to make wheelchairs—with the idea of opening a wheelchair shop in Michoacan and training others.
Also the idea of the Network or “RED” has been taken up and is being spearheaded by other groups, with the help of the NGO ‘VAMOS’ in Mexico City. At last CBR seems to be taking off in Mexico!
Announcements
Life After Injury by Liz Hobbs et al.
An excellent new handbook about the management, therapy, and ways of coping with traumatic injury (including landmine trauma). Introduction by David Werner. See enclosed flyer, or our site: www.healthwrights.org.
Politics of Health Knowledge Network
HealthWrights’ new interactive website, which analyzes the man-made and macroeconomic causes of poor health, and explores healthier, more equitable alternatives. See www.politicsofhealth.org.
PROJIMO Spanish Language Training Program
The intensive Spanish language training program taught by disabled instructors at PROJIMO is a great way to learn the language and volunteer in a unique community-based program. See the flyer or e-mail: PROJIMO_AC@hotmail.com
How You Can Help
Workshop Construction Volunteers
Volunteers with building skills or simply willing to work hard are needed for help in the construction of PROJIMO Duranguito’s new workshops, using innovative, bio-friendly architecture.
Contribute to Our Politics of Health Website
Help with Politics of Health Website is very much needed. We need help with everything from collecting information to organizing data, to website management. Volunteer from your home. Contact Shefali Gupta at shefali@politicsofhealth.org.
Spread the Word About Our Spanish Language Program
Spread the word about PROJIMO’s Spanish language training program, and help recruit students. This will help generate income for the program and the disabled instructors.
Make a Donation
Please make a donation. These groundbreaking activities urgently need funding assistance, to help others help themsleves.
End Matter
Please Note! If you prefer to receive future newsletters online, please e-mail us at: healthwrights@igc.org

| Board of Directors |
| Trude Bock |
| Roberto Fajardo |
| Barry Goldensohn |
| Bruce Hobson |
| Donald Laub |
| Eve Malo |
| Myra Polinger |
| Leopoldo Ribota |
| David Werner |
| Jason Weston |
| Efraín Zamora |
| International Advisory Board |
| Allison Akana — United States |
| Dwight Clark — Volunteers in Asia |
| David Sanders — South Africa |
| Mira Shiva — India |
| Michael Tan — Philippines |
| María Zúniga — Nicaragua |
| This issue was created by: |
| David Werner — Writing and Photos |
| Efraín Zamora — Technical Assistance |
| Shefali Gupta — Technical Assistance |
| Trude Bock — Proofreading |
| Dana Gundling — Proofreading |
It is not a sign of good health to be well adjusted to a sick society.
— J. Krishnamurti (1895-1986)